

Background: In patients with newly-diagnosed multiple myeloma (NDMM) who receive frontline autologous stem cell transplantation (ASCT), maintenance therapy (MT) following ASCT has been shown to delay disease progression and death. Current National Comprehensive Cancer Network (NCCN) guidelines also recommend MT for patients with MM, including the use of lenalidomide, bortezomib-based regimens, or ixazomib. However, there is limited evidence on the use and outcomes associated with MT in contemporary real-world patients. The present study assessed MT treatment patterns and clinical outcomes in a real-world US cohort of patients with NDMM following ASCT.
Methods: This retrospective, observational cohort study included NDMM patients initially diagnosed from 2011-2018 who received frontline ASCT. Patients were selected from the US Flatiron Health (FH) deidentified electronic health record (EHR)-derived database, which includes longitudinal patient-level data from over 265 community-based and academic cancer clinics across the US. To ensure capture of post-ASCT consolidation and MT, the study sample was restricted to patients who resumed contact within the FH network within 60 days following ASCT. Patients were excluded if they received treatment within the context of a clinical trial or had a second transplant within 180 days of their initial ASCT. Patients were classified as receiving MT if (during the 180-day post-transplant period) they initiated treatment with an NCCN-recommended MT regimen or continued to receive a subset of the antimyeloma agents used as induction regimen following ASCT and consolidation (if any). Key measures included baseline demographic and clinical characteristics, antimyeloma treatments (frontline induction, consolidation, and MT, if any), and clinical outcomes (time to next myeloma treatment [TTNT] and overall survival [OS]). Treatment duration and clinical outcomes were analyzed using Kaplan-Meier estimators and Cox regression to account for right-censoring. For TTNT and OS, follow-up began on the earlier of the ASCT date + 90 days or start of MT and continued through the dataset cut-off date (May 30, 2020) or loss to follow-up; TTNT and OS were estimated for patients receiving lenalidomide maintenance [R-MT], bortezomib maintenance [V-MT], or no MT, but was not estimated for other MT regimens due to sample size considerations.
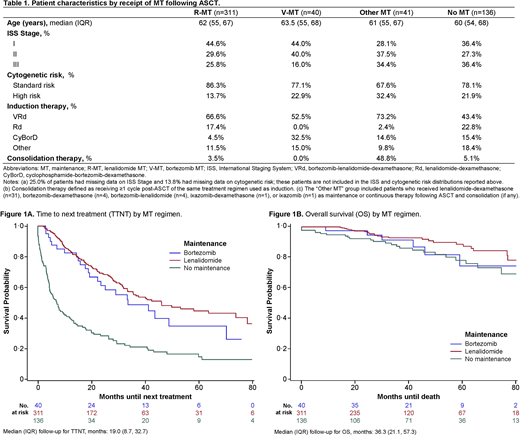
Results: 528 NDMM patients (median age 61 years, interquartile range [IQR]: 55, 68; 45.3% female) underwent ASCT and met study inclusion criteria. The most common induction regimens were bortezomib-lenalidomide-dexamethasone (VRd; 60.0%), lenalidomide-dexamethasone (Rd; 16.3%), and cyclophosphamide-bortezomib-dexamethasone (CyBorD; 10.2%). Following ASCT, 7.2% of patients received consolidation therapy and 74.2% received MT (lenalidomide monotherapy [R-MT]: 58.7%; bortezomib monotherapy [V-MT]: 7.6%; other MT: 7.8%). Median duration of MT was 18.0 months (IQR: 8.7, 29.1), and was similar for R-MT and V-MT (median 18.9 and 18.6 months, respectively). MT use increased from 69.3% to 79.0% from 2011-2013 to 2017-2018 (P=0.04); in addition, patients were more likely to have received VRd as induction across different MT (Table 1). R-MT and V-MT were both associated with longer TTNT relative to no MT (unadjusted hazard ratios [HRs]: 0.29 [95% CI: 0.22, 0.38] and 0.39 [95% CI: 0.25, 0.61], respectively) (Figure 1A). Improvements in OS were marginally significant with R-MT (HR: 0.58 [95% CI: 0.33, 1.00]) and nonsignificant with V-MT (HR: 0.86 [95% CI: 0.35, 2.11]) relative to no MT (Figure 1B); however, the OS estimates are characterized by low precision due to the relatively small number of events observed. Limitations included lack of documentation of reasons for treatment in the FH database, and use of consolidation and MT were inferred from observed treatment patterns; therefore, misclassification of MT was possible.
Conclusions: This analysis demonstrates that MT use following ASCT has increased in routine clinical practice in the US since 2011-2013, with R-MT being the most common regimen followed by V-MT. However, a substantial proportion of patients did not receive MT. MT use in real-world settings was associated with longer TTNT and a trend toward longer OS. Exploration of additional maintenance regimens to improve clinical outcomes is warranted in this patient population.
Ammann:Janssen Scientific Affairs: Current Employment, Current equity holder in publicly-traded company. Lam:Janssen: Current Employment. Tang:Janssen: Current Employment. Kampfenkel:Janssen: Current Employment. Sharma:Mu Sigma: Current Employment; Janssen: Other: Contractor. Lee:Janssen: Current Employment. Kaila:Janssen Scientific Affairs: Current Employment. Fu:Janssen: Current Employment. Gray:Janssen: Current Employment. He:Janssen: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal